After a few hiccups with Byron's Insurance - Fidelis Managed Care Medicaid - we are approved! This means the surgery, the hospital, the surgeons and rehab are all going to be paid at 100%. We did learn from the surgeon's office that if the out of network doctor (who is one of the surgeons) was not approved, the doctor would perform the surgery for free. :)
We leave on Thursday afternoon and have rented an Airbnb on 140th street and Amsterdam until next Wednesday. After that we have some flexibility to rent for longer if need be.
Onwards!
Tuesday, October 31, 2017
Friday, October 13, 2017
We REALLY have a date!
Apparently all went well when Byron was presented to the surgical team yesterday. Byron has a a surgical date of November 3 at 7:30 am.
Here he is - his usual wacky and wild self!
Here he is - his usual wacky and wild self!
Wednesday, October 11, 2017
We Have a Date?
The surgeons office called with a tentative surgery date - Friday November 3, 2017. But nothing is real until Byron's case is presented tomorrow at 9:30 am. We will all stay tuned!
Tuesday, October 10, 2017
More info on today's meeting
During the meeting today, the surgeon gave us more details on the surgery, recovery, time in the hospital, etc.
Byron can expect to be in surgery for 6-8 hours. The surgery is done with a microscope. Byron will have a four inch hole that will be closed up with very tiny screws that the doctor showed to us. With these screws, Byron will still be able to go through an MRI, C scan, metal detectors etc. The bone will heal completely in three months.
Byron will be in ICU for 1-3 days and then in the hospital for another 3-10. Because we are looking to go to Blythedale in Westchester for rehab, he may be transferred there early as they can do most of the wound care etc.
The most common immediate side effect is a kind of placid demeanor with not much personality. This is due to the brain trying to reorient itself. And the doctor said that Byron could just wake up completely the same as he went in. This would be due to the fact that there is currently not much going on in the right side. The MEG test results showed there was no activity there at all when Byron read or moved his eyes or spoke, other than seizure activity, so that is a very good sign. And all the seizure activity is still originating from the right so that is very good.
The surgeon promised they would call us today with a date but that didn't happen. I will call them tomorrow to see what can be done about getting a date. The surgeon said that we can start with a date even before he is presented because even if they choose the VNS instead of the surgery, it would be the same team. What we didn't make completely clear is that if the team is only willing to do the VNS, we will go to NYU for another opinion. As the team is not the ones seeing the regression as we do, we can't possibly wait the 8-10 months that the VNS will take to work. And as the surgeon said, we may end up here again in a year with a VNS failure. The thing that makes me nervous is he strongly recommended the surgery last year when Byron was presented but the neurologists convinced everyone that we needed to try more drugs first. So they do have some sway. Ah well - another two more days of waiting!
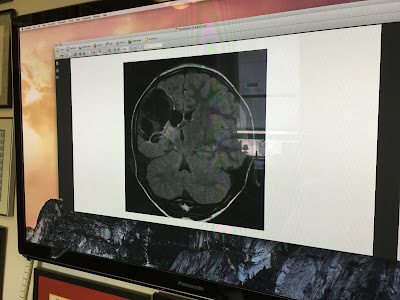
Below are some pictures he showed us of Byron's MRI. The white space that can be seen in the right hemisphere is fluid. According to the MRI , the left hemisphere is completely normal and seems to be doing all the good work.




Byron can expect to be in surgery for 6-8 hours. The surgery is done with a microscope. Byron will have a four inch hole that will be closed up with very tiny screws that the doctor showed to us. With these screws, Byron will still be able to go through an MRI, C scan, metal detectors etc. The bone will heal completely in three months.
Byron will be in ICU for 1-3 days and then in the hospital for another 3-10. Because we are looking to go to Blythedale in Westchester for rehab, he may be transferred there early as they can do most of the wound care etc.
The most common immediate side effect is a kind of placid demeanor with not much personality. This is due to the brain trying to reorient itself. And the doctor said that Byron could just wake up completely the same as he went in. This would be due to the fact that there is currently not much going on in the right side. The MEG test results showed there was no activity there at all when Byron read or moved his eyes or spoke, other than seizure activity, so that is a very good sign. And all the seizure activity is still originating from the right so that is very good.
The surgeon promised they would call us today with a date but that didn't happen. I will call them tomorrow to see what can be done about getting a date. The surgeon said that we can start with a date even before he is presented because even if they choose the VNS instead of the surgery, it would be the same team. What we didn't make completely clear is that if the team is only willing to do the VNS, we will go to NYU for another opinion. As the team is not the ones seeing the regression as we do, we can't possibly wait the 8-10 months that the VNS will take to work. And as the surgeon said, we may end up here again in a year with a VNS failure. The thing that makes me nervous is he strongly recommended the surgery last year when Byron was presented but the neurologists convinced everyone that we needed to try more drugs first. So they do have some sway. Ah well - another two more days of waiting!
Below are some pictures he showed us of Byron's MRI. The white space that can be seen in the right hemisphere is fluid. According to the MRI , the left hemisphere is completely normal and seems to be doing all the good work.





No date...yet
We arrived at the surgeons and he immediately told us Byron’s case had not been presented yet and would be on Thursday. He told us they were considering two options, functional hemispherectomy and the implantation of a Vagus Nerve Stimulator. I FREAKED out (a bit). The VNS has a low success rate and is rarely used in kids with as much brain damage as Byron. Midway through my speech Bob had to interrupt me and say rather forcefully, “Denise, he is agreeing with you!” Deep breath. Deep deep breath.
Bob and Dr. Feldstein really connected. They both make pens with a lathe and they compared their handiwork with photos and samples.
By the end of the visit we agreed that they would call us soon with a surgery date. The surgery would likely be early November and would likely be the Functional Hemispherectomy. So again, we wait. More soon. On the bus home now.
Bob and Dr. Feldstein really connected. They both make pens with a lathe and they compared their handiwork with photos and samples.
By the end of the visit we agreed that they would call us soon with a surgery date. The surgery would likely be early November and would likely be the Functional Hemispherectomy. So again, we wait. More soon. On the bus home now.
Tuesday, October 3, 2017
Appointments
Byron's appointment with the surgeon Dr. Feldstein will be on Tuesday, the day after Byron's case is presented to the surgical board. We should learn a lot in that appointment on Tuesday.
I confess I am a bit nervous. What I am hoping for is that Byron is approved for the Functional Hemispherectomy on Monday and the appointment on Tuesday is to discuss logistics, outcomes, and to make a plan. What I do not want to happen is that they either postpone again for some other intervention that is likely not to work, or suggest a much lesser surgery. The reason why I do not want the latter is that from everything I have read, including the scholarly articles I can get my hands on, is that these "Lobectomies" or partial surgeries have a very low cure rate and the Hemispheretcomy ends up needing to be done down the road anyway. They may err on the side of caution with this due to their fear that Byron will lose some critical functionality, but that caution may be specific to this hospital. The Cleveland Clinic, one of the top places to have this surgery in the world, weighed in on Byron's case last year. The Dr. there said they would not hesitate to go immediately to the Functional Hemispherectomy and that this was the best course of action. We can't choose this hospital however, because Byron's insurance is limited to New York based hospitals.
So we are very much hoping that from here on in we have smooth sailing towards the cure that will give Byron the best possible life - seizure free!
I confess I am a bit nervous. What I am hoping for is that Byron is approved for the Functional Hemispherectomy on Monday and the appointment on Tuesday is to discuss logistics, outcomes, and to make a plan. What I do not want to happen is that they either postpone again for some other intervention that is likely not to work, or suggest a much lesser surgery. The reason why I do not want the latter is that from everything I have read, including the scholarly articles I can get my hands on, is that these "Lobectomies" or partial surgeries have a very low cure rate and the Hemispheretcomy ends up needing to be done down the road anyway. They may err on the side of caution with this due to their fear that Byron will lose some critical functionality, but that caution may be specific to this hospital. The Cleveland Clinic, one of the top places to have this surgery in the world, weighed in on Byron's case last year. The Dr. there said they would not hesitate to go immediately to the Functional Hemispherectomy and that this was the best course of action. We can't choose this hospital however, because Byron's insurance is limited to New York based hospitals.
So we are very much hoping that from here on in we have smooth sailing towards the cure that will give Byron the best possible life - seizure free!
Monday, October 2, 2017
Things are moving!!
Just heard from Dr. Akman's nurse that Byron's case is being presented to the surgical committee next Monday ( a required step before the surgery can be approved) and we are going to meet with the surgeon, Dr. Feldstein this week. When Byron's case was presented in January 2017 they determined that we needed to try more pharmaceutical interventions first, before surgery was considered. I asked if that was likely to happen this time and the nurse said, "Dr. Akman is very clear that surgery is the next step for Byron."
It is very strange to be excited about a surgery of this magnitude, but with everything that is happening right now (Byron forgot the word for "Banana" the other day) it is the best next step.
Ultimately the board did approve the surgery in March 2017, but Byron went into temporary remission so we postponed the surgery. In March, Byron's condition was not nearly as dire. So I might have always wondered "Did I do the right thing?" But now we are absolutely sure. No regrets - only looking forward.

It is very strange to be excited about a surgery of this magnitude, but with everything that is happening right now (Byron forgot the word for "Banana" the other day) it is the best next step.
Ultimately the board did approve the surgery in March 2017, but Byron went into temporary remission so we postponed the surgery. In March, Byron's condition was not nearly as dire. So I might have always wondered "Did I do the right thing?" But now we are absolutely sure. No regrets - only looking forward.

Subscribe to:
Comments (Atom)